
Last updated:
‘The Search for a Certain Cure: Doctors, Drunkards and Victoria's Committee of Inquiry 1901’, Provenance: The Journal of Public Record Office Victoria, issue no. 10, 2011. ISSN 1832-2522. Copyright © Susanne Davies.
This is a peer reviewed article.
During the latter half of the nineteenth century, in Britain, North America and the Australian colonies, a dramatic change occurred in the way in which habitual drunkenness was understood. Having long been regarded as a sin or a vice, habitual drunkenness was gradually recast as a disease, one requiring specialist treatment if its sufferers were to have any hope at all of being cured. This article considers how the debate over drunkenness and its treatment played out in Victoria. In particular, it focuses upon the formation and work of a committee which in 1901 was appointed to investigate and test the merits of various ‘alleged cures’. As its proceedings demonstrate, exactly what was to be involved in the treatment of inebriates was a matter of heated dispute. Contributions to the committee provide us with insights into the varying questions, views and issues involved in the debate and moreover highlight, often poignantly, the vulnerability of those who sought to be cured.
In 1901, the Victorian Government appointed a committee to inquire into ‘certain alleged cures’ for inebriety. The committee’s formation was a product of decades of growing concern and often heated public debate over the nature and effects of drunkenness in Melbourne and was welcomed by a wide range of people including medical practitioners, social reformers and entrepreneurial laymen. Upon learning of the committee’s activities, some individuals with first-hand experience of drunkenness were moved to write of their circumstances and hopes. Mr Heming of Carlton, for example, took the opportunity to introduce his wife to Chief Secretary William Trenwith in this brief but revealing letter:
Dear Sir, I see by The Age of the 3rd that you want some inebriate to experiment on. My wife is an inebriate. She would be a good one to try. She will take anything to try and get better. I have tried a few cures but they have proved failures.[1]
This letter along with other documentation relating to the committee’s origins, proceedings and findings now forms part of the collection of Public Record Office Victoria. Taken as a whole, the surviving correspondence, transcripts of evidence and reports provide an exceptional insight into the committee’s workings as well as the broader nature and dimensions of the debate over drunkenness in late nineteenth century Victoria. They attest to the tireless efforts and growing influence that medical professionals and some social reformers exercised in changing understandings of habitual drunkenness and its treatment. They also illuminate some notable differences in the perspectives, interests and agendas of those engaged in the debate. The despair of those with troubling personal experiences of drunkenness is also revealed, especially in letters to the committee. As Catharine Coleborne has noted, such personal contributions deserve examination as ‘rich sources of information about families, households, and the language used by ordinary people’ to describe their experiences and interactions with experts and institutions.[2] Despite the richness of these records, the work of the committee and even its very existence have been largely forgotten. However, as the following discussion illustrates, the views, questions and issues it canvassed still resonate today in public debates concerning drugs and drug users.
The Problem of Drunkenness
By the late nineteenth century, Victoria’s social reformers, politicians and doctors agreed that alcohol, or more specifically, some people’s propensity to over-indulge in it, was the cause of inestimable harm. ‘The problem of drunkenness and other social problems run into the other like the colours of the rainbow’, observed Wesleyan Minister Alexander Edgar.[3] In medical, legal and charitable discourses, drunkenness was routinely linked to crime, insanity, disease and death. Inebriety, especially on the part of husbands and fathers, was identified as a major contributor to family breakdown and poverty. Habitual drunkards were accused not only of failing to contribute to the economy, but of draining government and charitable coffers, for many resided at the public’s expense in gaols, lunatic asylums and hospitals. In 1899, Herbert Booth, the Commandant of the Salvation Army in Victoria voiced the concerns of many when he told a board investigating the treatment of habitual drunkards that ‘the Government ought to act’. In his view, the prevailing policy of locking up drunkards was thoroughly futile, a point he made by comparing their treatment with that of the mentally ‘disturbed’. As he put it:
the habitual and chronic drunk is as powerless and as mentally unhinged, by the temptation presented to him at the entrance of the drinking saloon, as is any maniac. Why does society reserve all its remedial measures for one class of its weaklings, while it has no better system for the other than the ever-recurring police cell?[4]
Victorians were not alone in being vexed by the problem of habitual drunkenness. It was a subject that had also inspired prolonged debate in Britain, America and the other Australian colonies, and developments in these places played an important role in informing debate and reform initiatives in Victoria. The temperance movements in Britain and America, for example, found expression in the formation of organisations such as the Melbourne Total Abstinence Society in 1842 and, four decades later, a local branch of the Women’s Christian Temperance Union.[5] Temperance campaigners sought to limit alcohol at the point of supply and earnestly warned Melburnians against ‘treading the dangerous paths of moderation which ha[d] led so many down to the abyss of excess’.[6]
The teetotaller’s conception of habitual drunkenness as a sin or a vice came to be rivalled by quite a different view in the latter half of the century. This emerging view reflected a medical perspective and was just ‘one part of a wider movement towards a scientific discourse on social problems’.[7] Within it, habitual drunkenness was re-defined as a disease and drunkards were re-cast as ‘inebriates’, as individuals beset by a mental and physical disease and thus requiring specialised, scientifically based treatment. In 1872, the introduction of the Inebriates Act provided clear evidence that the medical perspective was gaining influence. This law enabled licensed individuals to operate retreats for the specific treatment and cure of inebriates and also set out the means by which inebriates, upon their own request or that of a friend or relative, might be committed. The following year Dr Charles McCarthy, who had long campaigned for the establishment of such institutions, opened the colony’s first Inebriate Retreat at Northcote.[8] Concerns over his management of the retreat resulted in it being taken over by the government in 1889. Three years later, the government signalled its lack of commitment by refusing to save the debt-ridden facility from closure.
Familiar allusions to immorality and vice continued to colour political and popular perceptions of drunkenness and found expression in the ongoing neglect of those inebriates who could neither afford to pay for treatment in one of the private clinics that had emerged nor avail themselves of the various ‘cures’ being eagerly extolled by local entrepreneurs. The fact that the majority of habitual drunkards remained at the mercy of the criminal justice system prompted organisations which dealt first-hand with the effects of drunkenness to come together in 1898 for a series of conferences at the Melbourne Town Hall. In an attempt to break free of familiar deadlocks, discussion of the licensing laws and arguments for and against temperance were excluded from the agenda. A deputation representing the participants later urged Premier George Turner to ensure that habitual drunkards were treated differently from ‘ordinary’ drunks and criminal offenders. It recommended the establishment of inebriate asylums for the treatment of those who would otherwise be assigned to gaol, and the introduction of labour colonies for the ‘discipline and control of persons of drunken habits’.[9] Parliamentarian James Cook was most forthright, arguing that the treatment of habitual drunkards was not a question reserved for teetotallers and church people but rather ‘a political one’. ‘As the government existed for the benefit of the whole people’, he argued, ‘surely the treatment of these people was a matter for the Government’.[10] Ephraim Zox, one of Melbourne’s most tenacious and influential philanthropists and reformers, suggested an inquiry into the matter.[11] He assured the Premier that ‘good results would accrue’ if the government established ‘a retreat for the poorer classes’, but Turner remained unconvinced.[12] He doubted that any scheme set up to deal with chronic drunkards would be successful. This assessment partly reflected his personal views of drunkards as individuals lacking in responsibility and self-restraint. As he told the deputation:
He had no sympathy with the drunkard, or with those who could afford to get drunk and then went to the shelters for a night’s free lodging, only to go out again next morning to get drunk again.[13]
Despite his pessimism, Turner agreed to appoint a board to inquire into the matter. He did so, on the condition that some members of the deputation would volunteer their services to it. Zox and Dr William Maloney leapt at the opportunity and the following year the Zox-chaired board submitted its report. Unsurprisingly, it echoed the views of the deputation, describing the existing laws as being ‘altogether inadequate for the purpose of checking drunkenness’ and recommending instead the establishment of a government retreat for inebriates on French Island; one that would be similar to a labour colony with hard work and open air serving as the basis for reform.[14]
Over the next two years, these recommendations were the subject of furious campaigning. Zox and representatives from both houses of parliament called upon the Premier to act.[15] The public and private overtures of those who claimed to be able to treat or cure inebriates added weight to the cause. Some of the more entrepreneurial, no doubt sensing a business opportunity, directly approached the government with offers to provide either goods or services at a price. Following Turner’s resignation in February 1901, the prospects for change improved. In July, a resolution calling for the establishment of a state inebriate institution was unanimously passed by the Legislative Assembly and, five months later, Chief Secretary Trenwith announced that he would be appointing a committee to investigate the merits of various alleged ‘cures’ that had been brought to his attention.[16] A set of perplexing questions underscored this initiative. Could drunkenness be prevented or treated or cured? Was there a single means or many which might be employed to rectify the incorrigible behaviour of habitual drunkards? Who should be entrusted to oversee their treatment? And finally, and perhaps most importantly, did drunkards need to be willing participants in their treatment in order to be cured?
The Committee and the Curers
In 1898, Zox had urged that women be appointed to any Royal Commission that might be established to investigate drunkenness. In his view, women ‘had a great amount of common-sense’ and ‘might be able to tell them what others might not be able to’.[17] Trenwith, however, opted for a more conventional committee, appointing five men. They were parliamentarians John Billson and Malcolm McKenzie, medic Dr Clarence Godfrey who was an assistant to the Government Medical Officer, and two clergymen, Dr Strong and Dr Bevan, both of whom were well known for their liberal outlooks and their commitment to the welfare of the working class, the uneducated and the poor of Melbourne. The involvement of such notable men highlights the importance that was attached to the problem of drunkenness and more specifically to the work of the committee. Its responsibilities were multiple. The committee was empowered to accept formulas from across the world for testing, as well as to receive applications from individuals upon whom the cures might be tested. It was required to oversee the experimental testing of alleged cures, to report upon their merits and finally to form a view as to whether or not an Institute for Inebriates should be established.[18]
The committee identified as its starting point the increasing body of thought that conceptualised drunkenness not as a sin but as a ‘physical and mental disease’.[19] In its summary report of May 1902, it expanded upon this by noting:
The treatment of inebriates as merely part of the criminal procedures of the community is a method which belongs to the barbarians of the past… Whatever may be performed during a condition of drunkenness, inebriety as a habit is rather a disease than a crime. It may be a vice. It also is a distinct physical deterioration.[20]
The idea that drunkenness was primarily a disease also carried weight with the contributors to the inquiry who, in the main, belonged to one of two groups. The first group comprised medical practitioners with specific or general experience of treating alcoholics and who claimed scientific knowledge as their own. The second group consisted of a range of individuals who lacked medical qualifications but who advanced the merits of various treatments and drew upon the testimony of ‘reformed’ drunkards as proof of their claims.
Even before the committee had begun its work, relations between these groups were strained. The ardent advocate of one particular remedy likened himself to an early scientist and warned against being ‘influenced by the sneers or doubts of some of the medical profession, who, in accordance with strict medical ethics, are opposed to all remedies of a secret nature’.[21] Another correspondent who had worked with inebriates in institutional settings rejected the notion of a cure-all and described those who advocated them as ‘catch penny charlatans’ who, at the very least, were ‘destitute of experience and common sense’.[22] Dr John Creed, whose contribution to the committee was specially recognised in its final report, was well aware that such antagonisms might derail any possibility of serious reform. In June 1902, he advised the committee to distribute a progress report in order to ‘place non debatable matter before the public, get their confidence and be in a better position to speak strongly as to the cures’. He warned that should this not take place, ‘the legislative necessities w[ould] be lost sight of in the scrimmage which [was] sure to occur from the enmity aroused in disappointed people’.[23]
And it was certain that there would be many who would be disappointed. Offers of various cures, remedies and treatments were readily forthcoming and ranged from the vague and hopeful through to the exceptionally polished and overly optimistic. One of the fastest starters, and certainly the most precocious contender for the government’s attentions, was JPT Caulfield, a reformed alcoholic. His Caulfield Institute at Studley Park promised affluent inebriates ‘the comforts and cheerful content of a nice home’ as well as ‘all the liquor they require[d]’.[24] Caulfield attributed his own return to sobriety to an American cure, but, having ventured into the field of treating patients, he was eager to distinguish his views and techniques from those of other practitioners. Thus while he advocated the medical treatment of inebriety, he rejected the commonly held view that success required a lengthy period of confinement or restraint. Caulfield defined inebriety as a lesion of the tissue cells and nuclei and identified it as the ‘first disease’ caused by the poison that was alcohol. Inebriety, he argued, was ‘characterised by a craving for liquor, and by an increased tolerance to the action of the poison’. Only his cure promised success for, unlike other treatments, it employed remedies that ‘cured the necessity and desire for strong drink’ rather than treating the secondary diseases which affected the drunkard’s bodily organs.[25] Exactly how the desire to drink was curbed was spelt out in a letter written by his sister. It detailed how patients would be freely provided with alcohol while at the same time injected with a formula that induced nausea and vomiting. A few days of this experience took away the desire for drink. Combined with gentler methods such as baths and massages, the patient could be discharged within three to six weeks, having been prepared, as she put it, to ‘choose his own path’.[26]
Caulfield’s formula was merely one of many brought to the attention of the committee. Charles Hoinville forwarded a recipe of ‘sulph [sic] Berry, oil of peppermint, magnesia, nutmeg’, while William Philpott offered his ‘purely herbal’ cure – ‘plutina’.[27] Charles Graham was so confident of his formula that he sought to test it upon an unconsenting party, who would be cured ‘in spite of himself’.[28] Mark Johnson, who worked at the Clunes District Hospital, reported good results using the Hatherlow Remedy, which he thought to be closely related to the Keeley Remedy that was widely marketed in the United States.[29] The fact that the cure of habitual drunkenness had become an international affair was clearly evidenced in letters written by representatives of the Central Methodist Mission which operated the Bichloride of Gold Institute at Jolimont. They had bought the rights to formulas devised by two American doctors, Thompson and Hagey, and claimed the bichloride of gold treatment to be ‘by far the best yet discovered’.[30] A formula supplied by JP O’Shaughnessy who worked at the Yarra Bend Asylum amply illustrates the unfortunate mix of ingredients found in such cures. It consisted of chloride of gold and sodium, inuriate of ammonia, nitrate of strychnia, atropia, fluid extracts of anchoria and coca, glycerine and distilled water. A full treatment lasted from three to five weeks and consisted of the patient being given a teaspoon of the formula every four hours over several days, then resting for a short interval, prior to another round of administration.[31]
Lined up in opposition to the peddlers of potions were the advocates of suggestion and hypnosis. Both J Crawford and Madame Aushley expressed their desire to demonstrate the effectiveness of hypnotism in treating inebriety, the latter adding, ‘the more severe the test the better’.[32] In advancing a similar course of intervention, Mr Swan referred the committee to ‘the greatest European practitioners’ who ‘regard [inebriety] not as a physical disease but a psychical [one]’.[33] As J Crawford McDowell, a self-taught hypnotist who claimed some success in treating inebriates explained: ‘The suggestion sets a train of thought in motion – Takes it out of one groove and directs it into another.’[34] The most influential proponent of this approach was however far more qualified in terms of his background and his promises. Mr Creed was a medical practitioner, a member of the Legislative Assembly of New South Wales, and had twice served as the president of that state’s branch of the British Medical Association. Possessing greater status and experience than most, his testimony, especially his advocacy of the curative treatment of inebriates as practised in New South Wales, was highly regarded by the committee.[35] Creed was of the view that ‘in itself, the administration of drugs [was] practically impotent in the treatment of chronic inebriety’. If cure happened to follow the administration of a remedy, he argued, this was due not to the drugs but rather ‘the moral support and self confidence afforded to the subjects by suggestion’. Suggestion, he argued, could be powerful even without hypnosis. Ultimately what mattered most, he believed, was the intellectual power and force of character that an inebriate possessed. Had any remedies ever worked, he asked, in the case of ‘an easily led person’ devoid of any ‘active desire on his own part’ to be cured?[36]
Those in Need of a Cure
Creed’s question illustrates how, despite its reformist nature, the debate over inebriety never fully escaped the influence of earlier conceptions that linked drunkenness to immorality and wantonness.[37] Given prevailing notions of gender, it is hardly surprising that many considered women to be less amenable to cure than men. According to Dr Norton Manning, who was a leading figure in debates concerning the mentally ill, women ‘seemed to have a smaller outlook, and once down were always down’.[38] The chance of sobriety being reached and then maintained was generally seen as being closely related to the character and proclivities of the individual. Caulfield’s sister put it this way:
There is in reality no positive cure for drunkenness or alcoholism, but under favourable circumstances people of a certain temperament can be assisted in a great measure to overcome the evil, their success depends afterwards on their own resolution, self-respect, and the influences brought to bear on their surroundings and purpose of life.[39]
The common request that cures only be tested upon willing participants arguably had less to do with a well developed sense of ethics than with the belief that a desire to be cured was necessary for the treatment to be successful.
Correspondence to the committee confirmed that there were indeed individuals who possessed such a desire. A basket maker from Brunswick named Adamson pleaded ‘to be one to be cured’. He had tried for six months to ‘get off the drink’ and had failed.[40] Mrs Frauenfelder, who described herself as a ‘working woman’, wrote of her difficulty in abstaining, while Mr Rogers, a married man with two children and a permanent position, went into more detail:
I am not like the majority of men have a glass and then leave it alone. When I start I don’t know when to stop and of course lose my senses altogether. It is not an everyday occurance [sic]. Thank God. I can guarantee to keep away for a month or more for that matter but I wish to get rid of the craving for ever. I would take any kind of medicine to do so.[41]
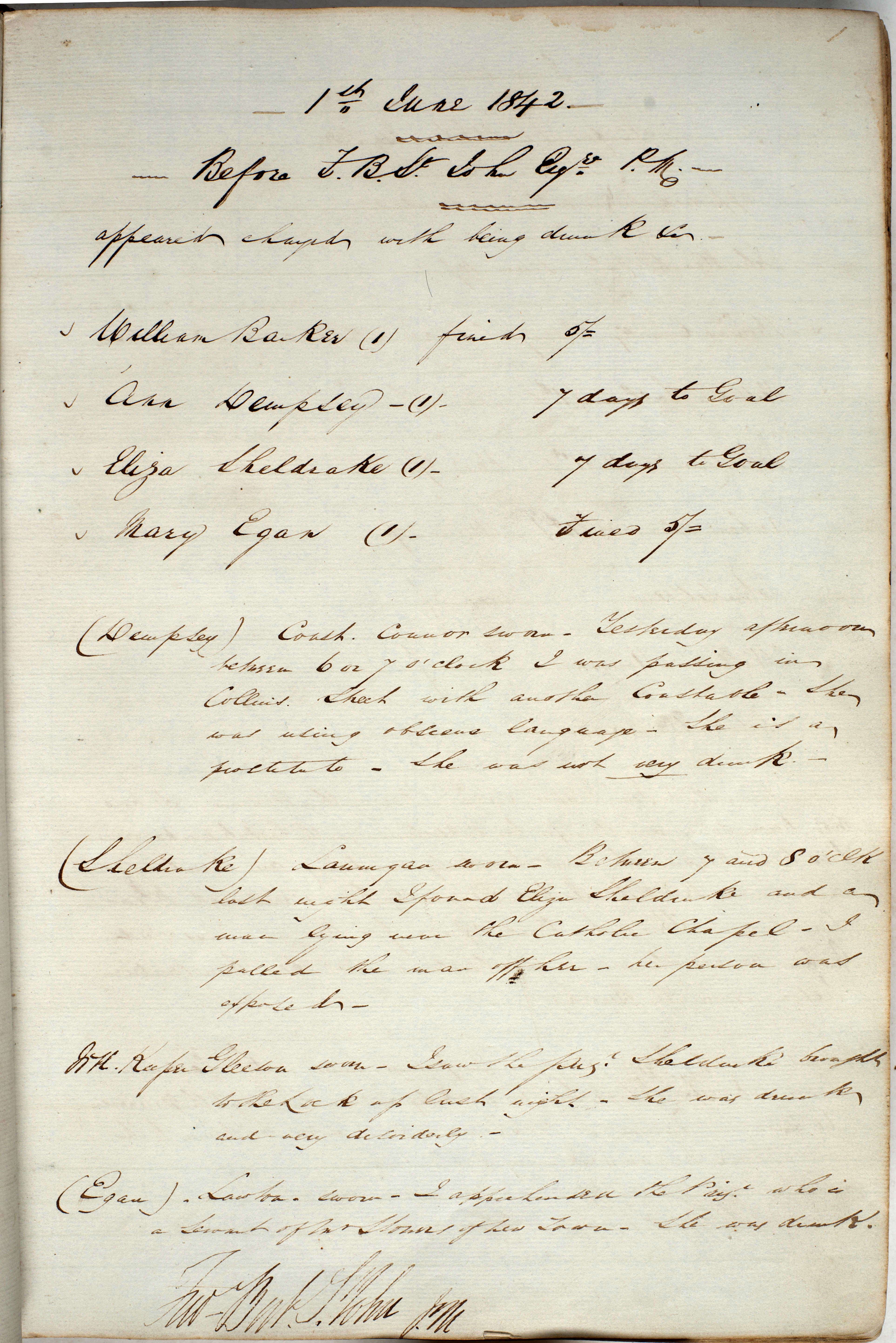
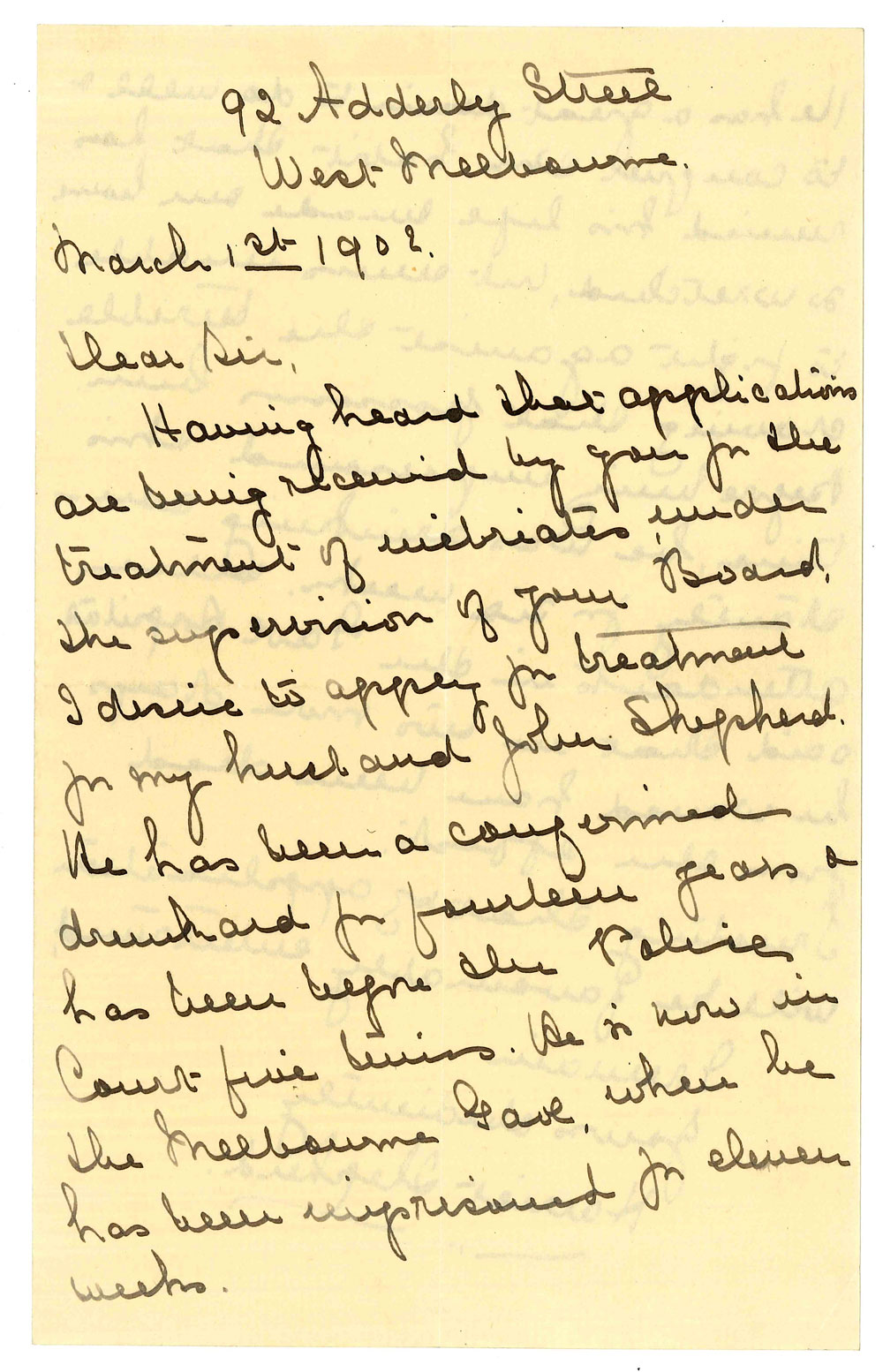
For every person who directly put themselves forward, there were two or three others who came to the committee’s attention via the efforts of people they knew. Dr Napthine offered his brother for cure, even though he held ‘no faith in such cures from a medical or scientific point of view’.[42] Miss Barton wrote of her brother whose addiction to drink, principally whisky, had caused ‘wretchedness to his wife’.[43] So too, no doubt, had the drinking of John Shepherd, who, according to his wife Harriet, had ‘been a confirmed drunkard for fourteen years and ha[d] been before the Police Court five times’. Shepherd had been drinking for six weeks prior to his latest arrest and when admitted to the Melbourne Gaol had reportedly been only a day or two away from death. In spite of all this, or perhaps because of it, Harriet felt able to write of her husband’s ‘great desire to do well, and to conquer this habit that [had] ruined his life and made [their] home so wretched’.[44]
It is not necessary to read between the lines of these letters to detect the deep shame and desperation felt by many of those affected either directly or indirectly by habitual drunkenness. Miss Barton, for example, recounted how when her brother was in the grip of cravings, there was nothing she or his wife could do or say to stop him. She did not want to mention their name however ‘as they were once well known’.[45] JP Eckert, a schoolmaster from Murtoa, was similarly wary of the damage that disclosure would do, and thus offered himself for cure only on the condition that his name not be released.[46] References to a reputable past or to a steady job were commonly offered as evidence of a good, or at least salvageable, character. William Stanley Philpott occupied the dual role of reformed inebriate and potential curer. He attributed his fall to ‘constant troubles followed by landbooming’, and had, he said, ‘passed through every stage of Delirium Tremens’. In attempting to interest the committee in his cure, Philpott expressed the hope that ‘men of practical experience (those who have passed the furnace)’ would control the cures rather than the beneficiaries of the patronage and friendship of ‘some in power’. This did not however prevent him from referring to the chair of an earlier government board as ‘an old friend’.[47] Despite his attempts to affirm his credibility, Philpott’s communications grew increasingly desperate in tone. Within five weeks of sending his first letter to Dr Bevan, he wrote to inform the committee that he was ill and staying at the Immigrant’s Home, an institution he described as being ‘very rough for [a] refined man’.[48] Over the course of the next month, Philpott wrote to both the Chief Secretary and the committee, correcting what he claimed to be public misrepresentations of his age and health, and growing increasingly insistent in his requests that he be provided with financial assistance given his ‘pennyless state’.[49]
Poverty was commonly cited not only as a consequence of drunkenness but also as a barrier to its treatment. WR Rogers thus felt the need to explain that ‘if required to go to an institution it would be impossible as I am only a poor man’.[50] Caulfield Institute with its promises of homely comforts, privacy, confidentiality and the ‘separate treatment for alcoholic ladies’ clearly catered for a more affluent clientele. The Bichloride of Gold Institute, operated by the Central Methodist Mission, opened its doors a little wider. According to its founder Dr Wolfenden, about 25 per cent of patients came in destitute and needed not only medical treatment but also food and clothing. It was a situation that had stretched the Institute almost to breaking point and thus he wrote to impress upon the committee ‘the urgent necessity’ of establishing a ‘state-aided institution for the treatment of those who [could] not afford to pay the necessarily high cost of private, separate treatment’.[51]
It was in fact this group which stood at the centre of the debate over habitual drunkenness. As Gerry Johnstone has noted in relation to the British experience, the better-off tippler whose drinking and treatment took place largely in private was overlooked.[52] Attention was instead focused upon those of lesser standing, whose drunkenness was more public. It was they, still tainted by notions of immorality and vice, who were blamed for the plethora of social ills that were linked to over-consumption. For the entrepreneurial set, this group also represented an opportunity. Providing them with services or goods on behalf of the government was liable to net a handsome profit, and thus offers of cures and treatment came accompanied with specific terms and conditions. G Ricketts, who ran a home for invalids and was already licensed under the Lunacy Act, offered a course of treatment lasting from three to six weeks and was willing to take in four or five patients at a time at a cost of £2 a week.[53] Charles Graham was less modest. He wanted £1000 for his formula should it be proven to work as well as a ‘salaried position at the hospital or retreat set up for inebriates’. The salary was ‘to be proportional to the benefits conferred’.[54] Caulfield was even more enterprising. He proposed that an institute be established and that, at a cost of £1500, he and the Caulfield Institute’s physician be appointed as the Superintendent and Chief Medical Officer respectively. In addition to these year-long appointments, all medicines were to be acquired from his company at a cost of £5 per patient and the government would be responsible for equipping the facility, providing all stores and paying for a matron and any servants required.[55] The representatives of the Bichloride of Gold Institute, like Caulfield, did not wish to sell their cure or their formula to the state, but expressed their interest in working with the government should it be decided that inebriates would be treated in ‘proper moral and hygienic surroundings’.[56]
Experimenting with Change
The fate of these proposals rested with the outcome of experiments that were to be overseen by the committee, but these proved difficult to organise. Dr Creed reacted with indignation when asked to give a display of the hypnotic cure of inebriety, for he considered it would be a gross breach of professional confidence.[57] Mr Swan preferred to try his cure outside of a gaol, and if it involved a woman he asked that a witness be present.[58] The representatives of the Bichloride of Gold Institute found the hospital at Pentridge Prison afforded a better environment for testing than the entirely unsuitable Melbourne Gaol, however neither facility in their view held acceptable candidates for cure. As they saw it, the prisoners at Pentridge ‘appeared in all cases to be criminals first and drunkards afterwards’, and as for the inmates at the Melbourne Gaol:
Most of the short sentenced prisoners were there for thieving, assaulting and other crime – the few who were drunkards were clearly persons of bad moral character or with no prospects or hope in life.[59]
In the surviving documentation there are fleeting references to what appear to have been experiments but it is impossible to know how many were conducted or what exactly they entailed. The only exception to this lies in an account of the testing of O’Shaughnessy’s cure upon eight ‘habitual drunkards confined in the Melbourne Gaol’. O’Shaughnessy had forwarded his formula free of charge and it was administered orally to the prisoners in treatments that lasted between two and nine days. In one case, testing had to be halted temporarily as a consequence of the prisoner’s ‘health’, and a check on the progress of the group a short time after the treatment showed mixed results. One of the men would still ‘take drink readily when offered’. Three had relapsed, including one who had been re-arrested for drunkenness within seven weeks of the treatment. Two were ‘fairly steady’ but not abstainers and the remaining two could not be traced. It was subsequently concluded that the drugs were ‘well known cardiac and nerve tonics’, and that the results of the experiment suggested nothing more.[60]
In its final report, dated 3 April 1903, the committee noted the many difficulties it had encountered in the course of its inquiries. While appreciative of the efforts of the many reformed drunkards who had spoken on behalf of various cures, it found their testimonies to be ‘too uncertain to be of any value’. The statistical evidence provided to them had been ‘vague’ and it had been impossible to establish whether cures were permanent or not. The gathering of information, much of which was from interstate or overseas, together with the examination and testing of formulas had been time-consuming. But even more problematic had been the fact that the ‘proprietors’ of the ‘best known and most popular cures’ were unwilling to divulge the specifics of their formulas.[61] For all its efforts, the committee was unable to affirm the existence of any specific and certain cure. It did however feel able to confirm that there were methods of treatment used in various institutions which resulted in the ‘restoration’ of large numbers of inebriates. These methods, it found, combined the administration of medicines with ‘physical and moral conditions’. Citing the example of New South Wales legislation, which it described as providing the ‘highest mark of restrictive and restorative action’, the committee called upon the government to act. As it put it,
For any civilized community to remain inactive or satisfied with a merely criminal treatment of the subject is to be guilty of a grave neglect, and almost justifies a charge of criminality upon the State itself.[62]
For reasons that remain unknown, the committee’s final report was never formally tabled in parliament. This may help to explain why its work has been largely overlooked by later generations. Still, it does appear to have had some effect, for in 1904 Victoria passed a new Inebriates Act. This legislation incorporated existing provisions allowing for the compulsory and voluntary confinement of inebriates in government licensed institutions, but also extended the powers of police and magistrates. Under the new law, a magistrate could order an individual convicted of three drink-related offences within a single year to be detained in a licensed institution for up to twelve months. Rather than simply being imprisoned, habitual drunkards were to be treated, but as is so often the case, the policy was not matched by an equal commitment of resources. Discreet facilities for inebriates were not immediately forthcoming, with the result that those who were committed as inebriates found themselves consigned to asylums intended for the treatment of the mentally ill. This outcome illustrates the difficulty of securing policy reform, especially when it concerns individuals or practices that are commonly regarded as being problematic or suspect. The questions and issues that were raised in the furore over habitual drunkenness remain important, for they set the contours and parameters of debates that continue to rage today.
Endnotes
[1] PROV, VA 4942 Royal Commission into the Treatment of Inebriates, VPRS 2598/P0 Records Relating to the Royal Commission…, Unit 1, Letter from W Heming to Mr Trenwith, 4 December 1901.
[2] C Coleborne, Madness in the family: insanity and institutions in the Australasian colonial world, 1860-1914, Palgrave Macmillan, Basingstoke, 2010, pp. 151-2. For a discussion of the value of information about the treatment of the mentally ill captured specifically within archival sources, see also C Colebourne, ‘Reading Insanity’s Archive’: Reflections from Four Archival Sites‘, Provenance, no. 9, 2010.
[3] Evidence of A Edgar in ‘Report of the Board appointed to inquire into the question of the treatment of habitual drunkards, with appendices and synopsis of evidence’, Victorian parliamentary papers, Session 1899-1900, vol. 4, 1899, no. 49, p. 34.
[4] Evidence of HH Booth in ibid., p. 29.
[5] A Hyslop, ‘Temperance, Christianity and feminism: the Women’s Christian Temperance Movement of Victoria, 1887-97’, Historical studies, vol. 17, no. 66, April 1976, pp. 28-30.
[6] These are the words of JW Meadon and were delivered at a Temperance Convention held in Melbourne in 1888. Quoted in D Dunstan, ‘Boozers and wowsers’, in V Burgmann & J Lee (eds), Constructing a culture, McPhee Gribble/Penguin, Fitzroy, 1988, p. 118.
[7] S Garton, ‘“Once a drunkard always a drunkard”: social reform and the problem of “habitual drunkenness” in Australia, 1880-1914’, Labour history, no. 53, November 1987, p. 53. For a further discussion of the re-definition of habitual drunkenness in other places see EM Brown, ‘“What shall we do with the inebriate?”: asylum treatment and the disease concept of alcoholism in the late nineteenth century’, Journal of the history of the behavioural sciences, vol. 21, January 1985, pp. 48-59.
[8] McCarthy firmly believed that chronic drunkenness was a medical issue and that its treatment was a government responsibility. He aired this view as early as 1859 in anonymous correspondence published in the Argus. See AM Mitchell, ‘McCarthy, Charles (1814-1896)‘, in Australian dictionary of biography online.
[9] PROV, VPRS 2598/P0, Unit 1, ‘The treatment of drunkards’, Deputation to the Premier, 9 September 1898.
[10] ibid.
[11] Ephraim Zox was a financier, philanthropist and politician. He chaired Royal Commissions into Victoria’s asylums (1884-86) and charitable institutions (1890, 1891, 1895) and also played a major role in various organisations including the Discharged Prisoners Aid Society. See LE Fredman, ‘Zox, Ephraim Laman (1837-1899)’, in Australian dictionary of biography online.
[12] PROV, VPRS 2598/P0, Unit 1, ‘The treatment of drunkards’, Deputation to the Premier, 9 September 1898.
[13] ibid.
[14] ‘Report of the Board appointed to inquire into the question of the treatment of habitual drunkards’, 1899, pp. 5, 12-13.
[15] ‘Habitual drunkards’, The Argus, 14 October 1899, p. 15.
[16] ‘State Inebriate Institute’, The Argus, 3 December 1901, p. 6.
[17] PROV, VPRS 2598/P0, Unit 1, ‘The treatment of drunkards’, Deputation to the Premier, 9 September 1898. All further references to correspondence and findings of the committee are from this collection.
[18] ‘Committee to report on certain alleged cures for inebriety’, remarks of the Chief Secretary to members of the committee, 20 December 1901.
[19] ‘Report of the Committee of Inquiry as to certain alleged cures for inebriety’, 9 April 1903.
[20] ‘Summary report of the Committee of Enquiry as to certain alleged cures for inebriety’, 6 May 1902.
[21] JPT Caulfield to Hon. JR Dickson, 30 October 1899.
[22] JP O’Shaughnessy to Chief Secretary, 21 November 1901.
[23] Dr Creed to Dr Bevan, 26 June 1902.
[24] JPT Caulfield to Chief Secretary, 16 January 1900.
[25] ibid.
[26] Miss C Caulfield to Chief Secretary, 16 October 1901.
[27] C Hoinville to Mr Trenwith, 31 December 1901 and WS Philpott to Dr Bevan, 21 December 1901.
[28] CH Graham to Chief Secretary, 17 December 1901.
[29] M Johnson to Dr Bevan, 12 July 1902.
[30] AR Edgar and AJ Derrick to AE Scott, 16 January 1902.
[31] JP O’Shaughnessy to Chief Secretary, 21 November 1901.
[32] J Crawford to Scott, 28 February 1902; Madam Aushley to Dr Bevan, 23 January 1901.
[33] Mr Swan to Rev. Dr Strong, 21 August 1902.
[34] J Crawford McDowell, Item VI, ‘Synopsis of evidence relating to the treatment of inebriety by hypnotism’.
[35] ‘Report of the Committee of Inquiry as to certain alleged cures for inebriety’, 9 April 1903.
[36] Dr Creed to Dr Bevan, 10 January 1902.
[37] See G Johnstone, ‘From vice to disease? The concepts of dipsomania and inebriety, 1860-1908’, Social and legal studies, vol. 5, 1996, p. 38.
[38] Norton Manning MD, Item V, ‘Synopsis of evidence mainly relating to the treatment of inebriety in general practice’.
[39] Miss C Caulfield to Chief Secretary, 17 October 1901.
[40] Letter from L Adamson, 5 December 1901.
[41] Letter from WR Rogers, 15 December 1901.
[42] Letter from Dr Napthine, 17 December 1901.
[43] Letter from Miss R Barton, 2 January 1902.
[44] Letter from H Shepherd, 1 March 1902.
[45] Letter from Miss R Barton, 2 January 1902.
[46] JP Eckert to Chief Secretary, 4 December 1901.
[47] WS Philpott to Dr Bevan, 21 December 1901.
[48] Philpott to Scott, 4 February 1902; Philpott to Chief Secretary, 5 February 1902.
[49] Philpott to Chief Secretary, 5 February 1902 and 17 February 1902; Philpott to Scott, 18 February 1902; Philpott to Dr Bevan, 1 March 1902.
[50] WR Rogers, 15 December 1901.
[51] J Wolfenden to Chief Secretary, 6 April 1900.
[52] Johnstone, ‘From vice to disease?’, p. 41.
[53] G Ricketts to Chief Secretary, 9 December 1901.
[54] CH Graham to Chief Secretary, 17 December 1901.
[55] JPT Caulfield to Chief Secretary, 16 January 1900.
[56] AR Edgar and AJ Derrick to AE Scott, 16 January 1902.
[57] Dr Creed to Dr Bevan, 14 June 1902.
[58] C Strong to Dr Scott ‘re. Swan’s hypnotic treatment & experiments’.
[59] AJ Derrick to Captain Evans, 6 December 1901.
[60] Minutes of meeting held at the residence of Dr Bevan, 6 May 1902, Item XII, ‘Minutes of evidence’.
[61] ‘Report of the Committee of Inquiry as to certain alleged cures for inebriety’, 9 April 1903.
[62] ibid.
Material in the Public Record Office Victoria archival collection contains words and descriptions that reflect attitudes and government policies at different times which may be insensitive and upsetting
Aboriginal and Torres Strait Islander Peoples should be aware the collection and website may contain images, voices and names of deceased persons.
PROV provides advice to researchers wishing to access, publish or re-use records about Aboriginal Peoples