
Last updated:
‘“Made enquiries, can elicit no history of injury”: Researching the History of Institutional Abuse in the Archives’, Provenance: The Journal of Public Record Office Victoria, issue no. 6, 2007. ISSN 1832-2522. Copyright © Lee-Ann Monk.
This is a peer reviewed article.
Recent public inquiries into the policies and practices of indigenous child removal and the institutionalisation of children more generally have revealed, through the often-harrowing accounts of those who experienced it, that abuse was a significant, if hidden, dimension of institutional life. These revelations demonstrate that a full understanding of the history and legacy of past institutions requires researchers to acknowledge and investigate institutional abuse.
The purpose of this article is to show the kinds of archival records and methods researchers might use to investigate institutional abuse, in the absence of testimony from survivors or other witnesses, taking as a case study the first twenty-five years in the history of the Kew Idiot Asylum (better known in Melbourne by its later name, Kew Cottages). The article shows that, while there are limitations to what we can now know, it is possible to see behind contemporary public assurances that all was well and discover the existence of institutional abuse, the forms it took, the circumstances in which it occurred and understandings of it within a particular institutional world.
Readers should be aware that the language used in the late nineteenth and early twentieth centuries to describe people with intellectual disability is now highly offensive. While acknowledging that this is so, this article retains the use of contemporary terms because they are revealing of past attitudes to, and understandings of, intellectual disability. Use of such terms has, however, been minimised where possible. The author would also like to stress that she does not share the assumptions the contemporary language expresses. The names of all patients and their families in this article are pseudonyms.
On 10 January 1906, the Senior Medical Officer at the Kew Idiot Asylum, Dr AA MacFarlane, was on his usual ‘morning round’ of the institution when he came upon Nurse Dowden assaulting patient Gwen Evans.[1] MacFarlane recorded the incident in Gwen’s case history, where it stands as a rare example of a documented instance of abuse. The exact nature of the assault he witnessed remains unclear, however, because an inkblot obscures significant parts of the entry. The difficulty of knowing exactly what happened in this instance is emblematic of the methodological and interpretative problems of researching abuse from archival sources. Despite these difficulties, such research is crucial to understanding the history and legacy of institutions. Abuse was a significant, though often hidden, aspect of institutional life, as the frequently harrowing stories of people who lived in institutions reveal.[2] The purpose of this article is to show the kinds of archival records and methods researchers might use to investigate institutional abuse in the absence of such testimony and what these can (and cannot) reveal about a particular institutional world. It uses as a case study the first twenty-five years in the history of the Kew Idiot Asylum, now better known by its later name, Kew Cottages. Abuse – ill-treating or acting injuriously toward an individual – can take many forms. The focus of this article is on verbal and physical forms of ‘ill-treatment’, such as swearing at or striking patients.
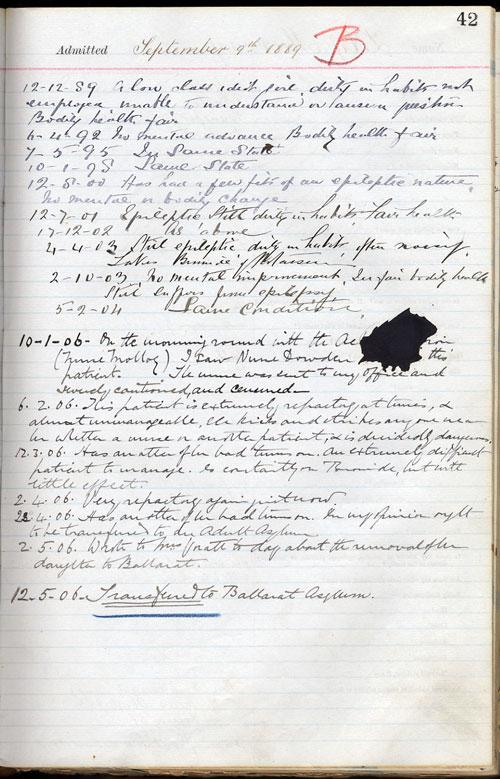
PROV, VPRS 7419/P1, Unit 1, 10 January 1906, p. 42.
Opened in May 1887, the Kew Idiot Asylum was Australia’s ‘first specialist institution’ for people with intellectual disability.[3] Dr Edward Paley, Victoria’s Inspector of Asylums, first suggested the establishment of a separate institution for ‘idiot children’ in 1875, when fifty-four such children were living in the colony’s ‘lunatic’ asylums. (At this time people with intellectual disability were commonly referred to as ‘idiots’ or ‘imbeciles’, in part to differentiate them from ‘lunatics’, as people with mental illness were known.) In Paley’s view, establishing a distinct institution for children had several advantages: it would allow them to be separated from the ‘adult insane’ with whom they were living, a situation contemporaries considered harmful to the children’s welfare; it would create space in the overcrowded asylums for the mentally ill; and it would make it possible ‘to initiate a system of industrial training and occupation’ for the children.[4] This desire to establish ‘an institution for the care and training of feeble-minded children’ reflected the ‘positive optimism’ about the developmental potential of people with intellectual disability then prevalent.[5] However, it took until 1887 before such an institution was successfully established.
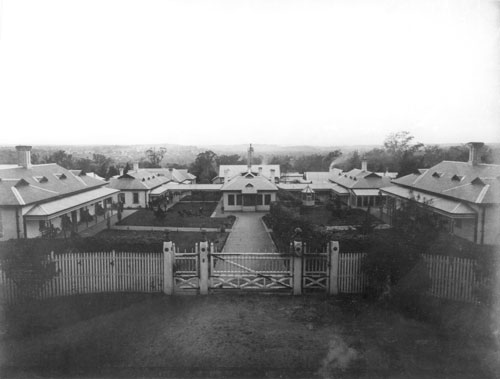
Courtesy of the Kew Cottages Historical Society.
For many families, the Idiot Asylum provided a release from the physical work and emotional distress of caring for their intellectually, and often physically, disabled children. A child’s violent behaviour, particularly toward other children, was the reason some families committed their son or daughter. Others sought institutionalisation to protect their children from potential dangers. Difficult economic circumstances seem to have precipitated some admissions, while other families hoped for improvement in their child’s condition.[6]
Built in the grounds of the Kew Lunatic Asylum, the Idiot Asylum was administratively part of Victoria’s Department of the Hospitals for the Insane (after 1905 renamed the Lunacy Department), in turn a Branch of the Chief Secretary’s Department.[7] The few institutional records that survive from the Asylum’s early history primarily concern the legal and medical management of patients. Among the most significant of these for a study of institutional abuse are patient case histories and the institution’s Medical Journals. The administrative relationship between the Lunatic and Idiot Asylums and their position in the public service hierarchy saw the creation of a handful of other relevant records. The most useful are the books in which the Inspector-General of the Insane (the administrative head of the Department under the minister) and Official Visitors noted their visits. Prior to the 1940s, the same Visitors were responsible for inspecting both the Lunatic and Idiot Asylums and wrote their observations in a single volume. Very few of the Lunacy Department records are helpful in researching abuse in the early part of the institution’s history. While the Department kept a Register of Complaints against Staff in all the asylums, the only extant volume dates from 1908. Much of the correspondence between the Asylum and the Inspector-General’s office is lost. However, correspondence from the Inspector-General to the Chief Secretary and the Department’s Annual Reports to parliament contain occasional references to institutional ill-treatment.
Case Books
Dr MacFarlane recorded the assault on Gwen in her case history. Legislation governing the asylums mandated the keeping of ‘Case Books’ in which the superintendent was to record ‘the mental state and bodily condition of every patient’ at admission and to keep a ‘history’ of the patient’s ‘case’ while in the asylum. A record of any medical or other treatment was also required, as was documentation of the cause of death, should the patient die.[8] The assault on Gwen is one of only two instances of ill-treatment found in 386 case histories sampled from the male and female patient Case Books 1887-1906.[9] While this frequency indicates that recording was rare, it is not indicative of the actual occurrence of abuse because, as the following discussion will show, the case histories do not record all instances of ill-treatment. Nonetheless, the few examples documented are revealing of the forms ill-treatment took, the circumstances in which it occurred and institutional understandings of it.
Gwen came to Kew from the Ararat Lunatic Asylum, where her mother admitted her in 1888, aged sixteen. The Superintendent at Ararat decided to transfer her to Kew the following year because she was not improving ‘mentally owing to the want of training facilities’.[10] Her subsequent case history reveals very little about her life at Kew. In compliance with legal requirements, the first entry, made roughly three months after her admission, records the Superintendent’s assessment of her mental condition and bodily health. Gwen’s subsequent case notes are extremely brief and infrequent, two or three years often elapsing between entries that say little more than that her ‘state’ remained unchanged, until MacFarlane recorded the assault upon her.
In marked contrast to these lengthy silences, a rush of entries follows (six in the space of four months). The first in this sequence, dated 6 February 1906, describes Gwen as ‘extremely refractory at times, and almost unmanageable. She kicks and strikes anyone near her whether a nurse or another patient and is decidedly dangerous’. Just over a month later, the Case Book records that Gwen had ‘another of her bad turns on’ and was ‘an extremely difficult patient to manage’. Medication was having ‘little effect’. In early April, she was said to be ‘Very refractory again’. Toward the end of the month, MacFarlane noted another ‘bad turn’, adding that she ‘ought to be transferred to an Adult Asylum’. In early May, he wrote to Gwen’s mother about her ‘removal’ to the Ballarat Asylum. Mrs Evans apparently raised no objection because the final entry in Gwen’s history records her transfer to Ballarat ten days later, a common fate for ‘refractory’ patients at Kew.[11]
This sequence of entries contextualises the assault. Gwen’s ‘refractory’ and ‘unmanageable’ behaviour and her violence toward other patients and staff provide clues about how the medical officers were likely to view Nurse Dowden’s actions. Legislation made it a misdemeanour to ‘strike wound ill-treat or wilfully neglect’ patients, punishable by a fine of not less than £2 and not more than £50 or imprisonment of not more than six months.[12] Departmental Regulations (written by the Inspector and approved by the minister), in force when the Idiot Asylum opened, made staff ‘liable to punishment for … ill-treatment of patients’. A revised set of Regulations, introduced in 1898, was even more explicit, deeming it ‘a grave offence for attendants to strike or ill-use patients, or to employ unnecessary violence toward them’. They also regulated staff use of bodily restraint and seclusion.[13] These Regulations apparently remained in force until at least 1910.
However, a brief reference to an instance of ill-treatment the year after Dowden’s assault on Gwen reveals that asylum officials recognised that patients who were difficult to manage might provoke staff to violence and considered such provocation a potentially mitigating factor. In his Annual Report for 1907, the Inspector-General, Dr W Ernest Jones, wrote that: ‘The conduct and general behaviour of the staff have been extremely satisfactory … One nurse was punished for slapping a patient under excessive provocation, but inflicting little or no injury. This nurse has since left the service.’[14] (An exhaustive search of all surviving case histories for patients admitted prior to 1908 found no record of this assault.) Clearly, in gauging the seriousness of an assault, officials also considered the degree of injury inflicted.
A departmental inquiry ‘into a charge against [an attendant] for striking a patient’ some six years later reveals that officials did deem the use of a degree of force acceptable, as implied by the prohibition of the use of ‘unnecessary violence’ in the Regulations. They also considered motivation important. On investigating, the Acting Inspector-General found that the attendant (as male staff were known) had ‘used an unnecessary degree of violence towards the patient and that it was intentional‘.[15] (Again, there is no record of this assault in the case histories or the Register of Complaints against Staff.)[16] The Lunacy Act 1903 granted asylum Superintendents the power to ‘reprimand or caution’ and, additionally, to fine staff up to a limit of £5. In instances where the Superintendent considered the offence sufficiently grave to warrant a report to the Inspector-General, he held the power to suspend staff and report them, after which an investigation by the Inspector-General followed. If the latter found the charges proved, he was authorised to ‘reduce’ the officer’s rank or salary or to withhold his or her yearly increments in pay, or leave owed, or to dismiss, provisional on the consent of the Governor-in-Council. In these cases, the officer would forfeit all salary or wages unless the Inspector-General ordered otherwise.[17] In this instance, the attendant was ‘reduced’ from the second to the third grade for a year (thus reducing his wages).[18]
These two cases (the 1907 slapping of a patient by the unnamed nurse and the intentional striking of a patient six years later) help to explain what may have happened to Gwen and the institutional understanding of it. Having caught Nurse Dowden assaulting her, MacFarlane sent Dowden to his office, where she was ‘severely cautioned and censured’.[19] Legally, this was the most lenient penalty available to him, suggesting that he did not consider the assault serious. Given his assessment of Gwen as ‘dangerous’ and ‘unmanageable’ (expressed in his notes and in the decision to transfer her to Ararat) it seems likely that he thought Dowden’s actions the result of provocation rather than an act of deliberate punishment. Perhaps he also thought a degree of force necessary to ‘manage’ Gwen. Moreover, it seems that he did not consider that she was seriously hurt; certainly, he made no note of injury in her case history. Documents record Dowden’s resignation three months later but the lack of any further detail makes it impossible to know whether her decision to quit related to the assault.[20]
In the same year that Dowden assaulted Gwen, Edward Allan alleged that staff had ‘ill-treated’ his son William. William was admitted to the Asylum from the Children’s Home in Flemington Road, North Melbourne, in April 1901, when he was almost eight years old. Again, the first entry in his case history records the Superintendent’s initial assessment of his mental and physical state, characterising him ‘A fair class imbecile boy, employed in workshops and attends school, in fair bodily health’. Subsequent entries are once more non-existent until June 1905.[21] William’s younger brother, Clarence, came from the Neglected Children’s Department to Kew five years later, aged seven.[22]
Four months later, the case histories of both boys note a series of visits by their father, Edward, which culminated in the following exasperated comment in William’s case notes:
Visited by his father this morning, he has been coming here every Sunday morning lately. Arriving at most irregular hours [on Sunday visiting hours were 9.30–11.00 am], sometimes at 12 and staying until 1.30 & 2 p.m, keeping his chidren [sic] away from their dinner, until he has been requested to leave. He has also complained that this boy has been sworn at, and ill-treated by the ‘Warders’ this is untrue, as the child is under the care of nurses at the Male Hospital[.]
MacFarlane made a similar note in Clarence’s history.[23] While these notes suggest that staff accommodated Allan visiting outside regular hours, they also express MacFarlane’s view of his behaviour as detrimental to his children. The implication that Allan was careless of his sons’ welfare subtly undermines his character, and so the credibility of the complaint that follows. Neither case history records any further reference to or investigation of his claims, reflecting MacFarlane’s rejection of them.[24] Not surprisingly, no other record of the complaint or of a subsequent investigation survives.
This lack of evidence makes it difficult to learn any more about the alleged ill-treatment and its circumstances. However, MacFarlane’s response is potentially revealing. He refuted Allan’s charges not by declaring that the ‘Warders’ (the term referred to the male attendant staff) would not swear at or ill-treat patients but by asserting that William was not in their care. This defence assumes that the ‘ill-treatment’ was very recent. While his case history confirms that William was ‘at the Male Hospital’ in early April 1906 (probably as the result of having a tooth extracted) and so under the care of nurses, by then he had lived at Kew some five years. That the note exists suggests that he was earlier living elsewhere in the institution than the Hospital. (A corresponding note on 4 July 1907 recorded that he was ‘to leave the Male Hospital’ that day.) While nurses cared for both girls and younger boys, an analysis of the admission histories of patients committed between 1906 and 1912 suggests that, at fourteen, William was too old to be living in the female division. A comparison of the age of patients with the wards to which they were assigned shows that the oldest male admission to the female division in these years was eight years old (it is not possible to do a similar analysis for patients admitted prior to 1906 because the Case Book does not record ward assignments.)[25] Analysis of the handful of transfers from the female to male division recorded in the case histories suggests that male patients were transferred to the latter between the ages of eight and twelve.[26]
Another instance of ‘ill-treatment’ lends credence to Edward Allan’s complaint that some staff in the male division treated patients less than gently. Michael Davies was admitted to Kew in November 1895 from the Industrial Schools, aged three. Eleven years later, in June 1906, his case history recorded his complaint to MacFarlane of ‘having been ill-treated’by an attendant ‘who caught him by the neck’. This entry is a rare account of a patient’s complaint of abuse. The last part of it describes the consequence of the attendant’s actions and is significant in being in Michael’s own words, MacFarlane noting verbatim his protest that the attendant ‘nearly broke my neck’.[27] MacFarlane considered Michael ‘one of the most intelligent boys in the Asylum’ and thought ‘he should be discharged, providing a suitable home could be provided for him’.[28] This assessment suggests that he was likely to consider Michael a credible witness.
Beyond revealing its existence, Michael’s complaint provides some sense of the forms ‘ill-treatment’ may have taken and a rare glimpse of everyday institutional practices, adding to the picture emerging from the cases already discussed. However, exactly what happened is again difficult to determine. Michael told MacFarlane that the attendant had ‘caught him by the neck’ and it seems likely that he meant the back of the neck rather than the throat. There is, in his complaint, a suggestion that it was not unusual to be so ‘caught’, because MacFarlane added an additional phrase (now difficult to decipher) that suggests that it was a subsequent action that resulted in Michael being injured. Michael’s complaint seems to be more an objection to the attendant’s apparent clumsiness or more-than-usual-roughness (the latter conveyed in his characterisation of the severity of the injury he suffered, the ‘nearly’ broken neck) rather than his first act of catching hold of him.
An episode some years later reinforces the impression that this may have been a commonplace method of control among attendants. In 1911, patient Gladstone Fletcher’s case history records that he ‘Threw stones at attends [sic] whom he accused of striking him’. The attendant in question denied that he had struck Gladstone, but admitted that he had ‘seized him by the neck to prevent him doing further damage’.[29] The attendant’s willingness to admit this (while denying striking Gladstone), suggests that he thought this an action the doctor would deem justified in the circumstances. The two cases suggest a possible continuity in attendants’ restraint practices, with individual warders resorting to similar methods of control over time.
Gladstone’s allegations of ill-treatment were dismissed in a concluding sentence that characterised him as ‘undependable & word cannot be accepted’. However, his admission notes, by revealing something of his response to ill-treatment outside the institution, lend weight to his allegations. In answer to the question ‘Whether dangerous to others’, they record: ‘Only if crossed: chases boys when they tease him & strikes them’. Case histories usually derive such information from committal documents. In Gladstone’s case, one of the medical certificates accompanying the request for his admission commented that he ‘fills his pockets with stones to throw at boys who annoy him’. On the day that he threw stones at the attendants, Gladstone’s ‘pockets’ were ‘found to be full of blue metal’.[30] Thus, his actions seem consistent with his earlier response to ‘annoyance’, suggesting that the attendants may well have struck or otherwise manhandled him.
His case history also suggests that he was a patient against whom attendants were more likely to use physical force. In September 1910 Dr Woinarski, the Junior Medical Officer, noted that Gladstone ‘Ought to be transferred to Main Building – undependable & frequently assaulting other patients, always smaller than himself’. Staff apparently attempted to prevent this behaviour, the next note recording that he remained ‘a source of annoyance to patients smaller than himself still despite rebukes’.[31] Given the characterisation of Gladstone as ‘dangerous’ when ‘crossed’, perhaps he interpreted these rebukes as ill-treatment. Alternatively, they may have taken physical form, the attendants in fact striking or otherwise physically restraining him (in the words of one to prevent him ‘from doing further damage’). While he was still acting violently toward other patients in June 1911, it was his stone throwing which saw him transferred to the ‘main’ Kew Asylum a few weeks later.[32]
No evidence survives to suggest that the Medical Officer punished the attendant in either this instance or after Michael Davies complained that the attendant seized him by the neck. No departmental inquiry or note of punishment appears in the Inspector-General’s Book or the Complaint Register. Any punishment inflicted was thus likely to have been lenient, perhaps akin to the caution meted out to Nurse Dowden after her assault on Gwen, suggesting that the medical officers did not consider seizing a patient by the neck serious ill-treatment. The attendant who allegedly ill-treated Michael resigned two weeks after the incident; again, surviving records give no clue to the reason.[33] The resignation date of the attendant who was the object of Gladstone’s stone throwing is unknown.
Nurse Dowden’s assault on Gwen, Edward Allan’s complaints about the ill-treatment of his son and Michael Davies’s protest all occurred within the space of a year. While there are no recorded instances of abuse in the Case Book sample prior to 1906, this sudden change is likely to be an effect of the differences in individual doctors’ record keeping rather than an actual increase in ill-treatment. MacFarlane, who noted these incidents, took charge of the Asylum in August 1905, replacing its first Superintendent, Dr James McCreery.[34] Careful examination of the sample of case histories written by each man reveal significant differences in the particulars they chose to document. One of the most important is McCreery’s failure to note family visits or correspondence between relatives and the institution. MacFarlane, in contrast, recorded both. It beggars belief that not a single relative chose to write enquiring after their loved one or visited the institution in its first eighteen years of existence. Moreover, a handful of surviving letters show that families did write and visit during McCreery’s superintendence.[35] Given this difference, it is not safe to assume that the Case Books’ silence reflects the absence of abuse prior to 1906. (Neither is it safe to assume that Gwen Evans was not a difficult patient to manage prior to Dowden’s assault or that Edward Allan did not visit his sons before late 1906.)
Medical Journals
The institution’s Medical Journals provide another potentially important source for the investigation of institutional abuse. Legislation required Superintendents to keep a weekly Medical Journal in which they were to enter, among other things, ‘every death injury and violence which shall have happened or affected any patient since the last preceding entry’.[36] The Medical Journals for the Idiot Asylum are extant from 1899 but a comparison with other documents reveals that they are not, in fact, a complete record. Neither the assault on Gwen, nor the slapping of the patient mentioned in the 1907 Annual Report, appear.[37] In fact, Michael’s complaint that the attendant seized him by the neck is the only incident of obvious ill-treatment recorded between 1899 and 1908.[38] Consequently, as with the case histories, the silence that predominates in their pages is not indicative of the absence of abuse.

Courtesy of the Kew Cottages Historical Society.
One alternative method of analysis is to examine the Journals for patterns of injury and deviations from those patterns. For example, Journal entries attribute many injuries to falls, slightly more than half of which were, in turn, said to be caused by ‘fits’.[39] Most seem minor (cuts to the head or chin) and, in an institution in which many patients (perhaps almost half) experienced seizures of some kind, unremarkable. The most striking exceptions in this pattern are the incidence of three broken collarbones in the decade between 1899 and 1908, all attributed to seizure-related falls.
The first occurred in December 1902 when patient Robert Martin reportedly fractured his ‘right clavicle by fall in fit’.[40] The second took place in November 1906, when MacFarlane noted that patient Chester Charles ‘fell in a fit and fractured his right clavicle’.[41] The third happened only six weeks later, in mid-January 1907, when MacFarlane recorded his discovery that patient John Neale had ‘a green stick fracture of Right Clavicle. Evidently happened during a fit’.[42] (The Macquarie Dictionary defines a green-stick fracture as ‘a partial fracture of a bone … in which only one side of a bone is broken’.) While each injury individually is not suspicious, the coincidence of the latter two and their severity, in comparison with other injuries attributed to seizure-related falls, do raise questions.
Other evidence confirms that their coincidence was unusual and the injury considered serious. In late January 1907, the Inspector-General paid one of his regular visits to the Asylum, writing in the Visitors’ book that he found ‘the wards clean and bright and the place in good order generally’. He noted, as he and the other Visitors often did, several patients confined to bed, adding, ‘beyond the fact that two male patients have sustained fractures of the collarbone from falls in fits, there is nothing unusual in the sick cases’.[43] Comparing the date of this entry with Chester and John’s histories confirms that they were the patients he observed; both were in the Male Hospital on the day of his visit.
The Inspector-General also considered their injuries sufficiently serious to include in his Annual Reports for 1906 and 1907. In 1906, he wrote that an unnamed patient had ‘fractured his right clavicle from a fall in an epileptic fit’.[44] The following year, he reported that ‘I.N. aet. [sic] thirteen, sustained a fractured clavicle (greenstick) in an epileptic fit’. (While the Inspector-General did not name the patient in 1906, and referred to the patient in 1907 by the initials I.N., the nature of the injuries suggest that he was almost certainly referring to Chester and John.) Of John’s injury and another (a severely cut wrist) he concluded that ‘no blame could be attributed to those in charge of the injured children’.[45] The Medical Journal, however, suggests that MacFarlane felt less sanguine. His remark that John’s injury ‘Evidently happened during a fit’ reveals that he was suspicious about its cause. However, the Journal provides no further clues about the circumstances in which it or the other fractures occurred and it is necessary to turn to the case histories to learn more.
John Neale was admitted to Kew in July 1906, aged thirteen, and was evidently a difficult patient. The entry for 25 July characterised him as ‘very incoherent and refractory, has had to be kept in bed since admission. Appears to know or understand very little’. In early January the following year, MacFarlane recorded his discovery that John had ‘a bruise over [his] R. Clavicle’, adding that it ‘evidently occurred in the night and probably in a fit. Made enquiries can elicit no history of injury’. Four days later, he found that John had actually sustained the ‘green stick fracture, had him removed to the Male Hospital, and set the arm’. The bone did not heal quickly and John remained at the Hospital a month later. In noting his subsequent transfer back to the ward, MacFarlane added that he was ‘an extremely troublesome boy to manage. Won’t stay in bed, gets up, walks about the ward, and exposes himself’. He was apparently still in bed in early March, but whether because of the fracture is unclear.[46]
Everything we know from the analysis of other incidents of ill-treatment increases the suspicion that John’s injury was not a result of falling during a seizure. That analysis shows that some nurses and attendants did use force on difficult or ‘refractory’ patients. Moreover, the fact that all but two of the actual or alleged instances of ill-treatment discussed occurred in the institution’s male division suggests that some male staff may have been more inclined to use a degree of force, if only to the extent of treating patients roughly, than their female colleagues. (Nurse Dowden’s assault on Gwen and the slapping of the patient mentioned in the 1907 Annual Report were the exceptions.) Given the leeway provided by the prohibition in Regulations of ‘unnecessary violence’, staff willingness to admit to some use of force in other cases and the official attitude that force was sometimes excusable or justified, MacFarlane’s failure to elicit any explanation from staff about how John was injured is significant. It suggests that his injury was not the result of an impulsive reaction to the provocation of a difficult patient, as in Gwen’s case, or a resort to rough-and-ready control, but closer to the ‘intentional’ and ‘excessive’ 1913 assault that resulted in its perpetrator being ‘reduced’ by the Inspector-General. Staff no doubt understood the continuum upon which the officers based their judgements, as the attendant’s concession that he had seized the stone-throwing Gladstone Fletcher by the neck, but had not struck him, suggests.
However, it is now extremely difficult to know exactly what happened that night in the ward to cause John’s injury. An examination of other cases of ill-treatment (as when the officers observed an attendant at the ‘main’ Kew Asylum drag a patient across the yard, push him ‘roughly’ into a chair and strike ‘him two distinct, wilful and forcible blows with his fist upon his chest and ribs’)[47] suggest how such injuries might occur. Similarly, analysis of patterns of injury across the asylums might show that attendants were using particular methods of illicit bodily restraint. (The relatively high incidence of broken ribs among nineteenth-century asylum patients is one example.)[48] Such comparisons, however, cannot prove definitively what happened to John.
This article sets out to demonstrate the kinds of records and methods researchers might use to investigate institutional abuse, using the first twenty-five years of the Kew Idiot Asylum as a case study. Limitations in the surviving records, such as the failure to record all (indeed, in the case histories before 1906, any) instances of ill-treatment make it impossible to calculate the extent of abuse in the institution. Despite their incompleteness, however, the documents show that instances of abuse did occur. ‘Refractory’ patients, those who resisted the routines of the institution or were otherwise difficult, were apparently more likely to be the victims of such ‘ill-treatment’. Moreover, officials seemingly judged the use of force more leniently if it seemed provoked by challenging behaviour, or necessary, where a patient seemed otherwise unmanageable. However, Michael Davies’s complaint that an attendant nearly broke his neck, Edward Allan’s protest that the warders were ill-treating his son and Gladstone Fletcher’s resort to retributive stone throwing suggest that use of force, or at least a degree of ‘rough handling’, may have been more common in the male division.
The failure to mention the ambiguous circumstances surrounding John Neale’s green-stick fracture in the 1907 Annual Report suggests that the Inspector-General was reluctant to admit publicly that staff may have ill-treated or injured patients. This omission shows that the reassurances of such public records, while comforting, are not always reliable. While it is often not possible to know now exactly what happened, it is possible by careful analysis of surviving records to see beyond such public assurances. To do so is critical to a better understanding of the history of institutions and their legacy in the present.
Endnotes
[1] Case history entry, PROV, VA 2852 Kew Cottages, VPRS 7419/P1 Case Books of Female Patients, Unit 1, 10 January 1906, p. 42.
[2] J Penglase, Orphans of the living: growing up in ‘care’ in twentieth-century Australia, Curtin University Books, Perth, 2005; Australian Senate Community Affairs References Committee, Forgotten Australians: a report on Australians who experienced institutional or out-of-home care as children, Community Affairs References Committee, Canberra, 2004; National Inquiry into the Separation of Aboriginal and Torres Strait Islander Children from their Families (Australia), Bringing them home: report of the national inquiry into the separation of Aboriginal and Torres Strait Islander children from their families, Human Rights and Equal Opportunity Commission, Canberra, 1997.
[3] C Fox, ‘”Forehead low, aspect idiotic”: intellectual disability in Victorian asylums, 1870–1887’, in C Coleborne & D MacKinnon (eds) ‘Madness’ in Australia: histories, heritage and the asylum, University of Queensland Press, St Lucia, 2003, pp. 145, 155.
[4] Report of the Inspector of Lunatic Asylums on the Hospitals for the Insane for the Year Ended 31st December 1875, Victoria. Papers presented to both houses of parliament, 1876, vol. II, p. 12.
[5] Report of the Inspector of Asylums on the Hospitals for the Insane for the Year 1887, Victoria. Papers presented to parliament, Session 1888, vol. III, Appendix C, p. 46; Fox, ‘”Forehead low, aspect idiotic”‘, pp. 153–5; D Gladstone, ‘The changing dynamic of institutional care: the Western Counties Idiot Asylum, 1864–1914’, in D Wright & A Digby (eds), From idiocy to mental deficiency: historical perspectives on people with learning disabilities, Routledge, London, 1996, pp. 138–9.
[6] For example, case history entry, PROV, VPRS 7419/P1, Unit 1, nd, p. 318; medical certificates Gertrude C, PROV, VA 2852 Kew Cottages, VPRS 7565/P1 Admission Warrants Male and Female Patients, Unit 1, 5 August 1891; medical certificate Elise N, Unit 3, 7 September 1901; medical certificate Rita D, Unit 4, 15 April 1908; case history entry, PROV, VPRS 7419/P1, Unit 1, 7 July 1900, p. 198.
[7] Lunacy Act 1903, s. 12 (1).
[8] Lunacy Statute 1867, s. 21; Lunacy Act 1890, s. 31; Lunacy Act 1903, s. 37.
[9] PROV, VA 2852 Kew Cottages, VPRS 7419/P1, Case Book of Female Patients, Unit 1 and VPRS 7420/P1 Case Book of Male Patients, Units 1 and 2.
[10] Direction to Remove from Current Lunatic Asylum Gwen Evans, PROV, VPRS 7565/P1, Unit 1, D89/772, 3 September 1889.
[11] Case history entries, PROV, VPRS 7419/P1, Unit 1, 6 February, 12 March, 2 and 23 April, 2 and 12 May 1906, p. 42.
[12] Lunacy Statute 1867, s. 189; Lunacy Act 1890, s. 257.
[13] Hospitals for the Insane, Regulations for the Guidance of Attendants in the Asylums for the Insane, PROV, VA 475 Chief Secretary’s Department, VPRS 3991/P0 Inward Registered Correspondence II, Unit 752, File 72/E2729, clause 3, p. 5 and clause 21, p. 6; Regulations for Attendants and Nurses, PROV, VA 475, VPRS 3992/P0 Inward Registered Correspondence III, Unit 723, Item 98/G7010, clauses 19 and 20, p. 5.
[14] Hospitals for the Insane, Report of the Inspector-General of the Insane for the Year ended 1907, Votes and Proceedings of the Legislative Assembly, Session 1908, vol. I, p. 21.
[15] Visitors’ Book entry, PROV, VA 2840 Kew Hospital for the Insane, VPRS 7468/P1 Inspector-General’s and Visitors’ Book, Unit 1, 4 August 1913, np, my emphasis.
[16] PROV, VA 2864 Lunacy Department, VPRS 7518/P1 Register of Complaints Against Staff, Unit 1.
[17] Lunacy Act 1903, s. 14, pp. 7–8.
[18] Visitors’ Book entry, PROV, VPRS 7468/P1, Unit 1, 4 August 1913, np.
[19] Case history entry, PROV, VPRS 7419/P1, Unit 1, 10 January 1906, p. 42.
[20] PROV, VA 2863 Hospitals for the Insane Branch, VPRS 7519/P1 Staff Registers, Unit 3; Memo, Inspector-General to Under Secretary, PROV, VPRS 3992/P0, Unit 1014, File 1906/X2308, 24 April 1906.
[21] Case history, PROV, VPRS 7420/P1, Unit 1, p. 287.
[22] Case history, PROV, VPRS 7420/P1, Unit 2, p. 56.
[23] Case history entry, PROV, VPRS 7420/P1, Unit 1, 4 November 1906, p. 287 and Unit 2, 4 November 1906, p. 56; Memo Inspector to Under Secretary, PROV, VPRS 3992/P0, Unit 915, File 1903/S1879, 17 March 1903.
[24] Case history entry, PROV, VPRS 7420/P1, Unit 1, 1 January 1907, p. 287 and case history entry, Unit 2, 2 January 1907, p. 56.
[25] PROV, VPRS 7420/P1, Unit 3.
[26] PROV, VPRS 7420/P1, Units 1-3 and PROV, VA 2852 Kew Cottages, VPRS 7449/P1 Clinical Notes of Male Patients, Unit 1.
[27] Case history entry, PROV, VPRS 7420/P1, Unit 1, 14 June 1906, p. 168.
[28] Case history entry, PROV, VPRS 7420/P1, Unit 1, 2 January 1906, p. 168.
[29] Case history entry, PROV, VPRS 7420/P1, Unit 3, 7 July 1911, p. 60.
[30] PROV, VPRS 7565/P1, Unit 4, Medical Certificate Gladstone Fletcher; case history entry, VPRS 7420/P1, Unit 3, 7 July 1911, p. 60.
[31] Case history entries, PROV, VPRS 7420/P1, Unit 3, 7 September and 20 October 1910, p. 60.
[32] Case history entries, PROV, VPRS 7420/P1, Unit 3, 18 June and 8 July 1911, p. 60.
[33] PROV, VPRS 7519/P1, Unit 3, p. 76.
[34] PROV, VPRS 3992/P0, Unit 996, File 1905/V4860.
[35] Letter, PROV, VPRS 3992/P0, Unit 920, File 1903/R3064, 14 May 1903 and Memo Under Secretary to Inspector, PROV, VPRS 3992/P0, Unit 924, File 1903/S4204, 9 July 1903; PROV, VPRS 7419/P1, Unit 1, letter from Karl S to the Matron, 4 October 1904, p. 272.
[36] Lunacy Statute 1867, s. 21 and Lunacy Act 1903, s. 37.
[37] PROV, VA 2852 Kew Cottages, VPRS 7431/P1 Medical Journals, Units 1–2.
[38] PROV, VPRS 7431/P1 Medical Journals, Unit 2, p. 175.
[39] PROV, VPRS 7431/P1 Medical Journals, Units 1–3.
[40] PROV, VPRS 7431/P1 Medical Journals, Unit 1, p. 413.
[41] PROV, VPRS 7431/P1 Medical Journals, Unit 2, p. 223.
[42] PROV, VPRS 7431/P1 Medical Journals, Unit 2, p. 237.
[43] W Ernest Jones, Visitors’ Book entry, PROV, VPRS 7468/P1, Unit 1, 24 January 1907, np.
[44] Hospitals for the Insane, Report of the Inspector-General of the Insane for the Year Ended 1906, Papers presented to parliament, 1907, vol. II, p. 19.
[45] Hospitals for the Insane, Report of the Inspector-General of the Insane for the Year Ended 1907, Votes and Proceedings of the Legislative Assembly, 1908, vol. I, p. 21.
[46] Case history entries, PROV, VPRS 7420/P1, Unit 2, 25 July 1906; 6, 10, 20 and 23 January, 8 and 17 February and 4 March 1907; p. 59.
[47] Memo, Medical Superintendent W Barker to the Inspector-General, PROV, VPRS 3992/P0, Box 1057, File 1907/A5567, 19 June 1907 and Memo, W Barker, 19 June 1907.
[48] N Tomes, ‘The great restraint controversy: a comparative perspective on Anglo-American psychiatry in the nineteenth century’, in WF Bynum, R Porter & M Shepherd (eds), The anatomy of madness: essays in the history of madness: the asylum and its psychiatry, vol. III, Routledge, London, 1988, pp. 198–9; pp. 220–1, note 31.
Material in the Public Record Office Victoria archival collection contains words and descriptions that reflect attitudes and government policies at different times which may be insensitive and upsetting
Aboriginal and Torres Strait Islander Peoples should be aware the collection and website may contain images, voices and names of deceased persons.
PROV provides advice to researchers wishing to access, publish or re-use records about Aboriginal Peoples